Reworked from Nutrition Network Certification Pathway assignment by Dr. Louise Phillips, MD
Reviewed by Tamzyn Murphy
The diagnosis of diabetes and prediabetes are made based on meeting specified thresholds of three tests, namely the oral glucose tolerance test (OGTT), fasting blood glucose level (FBG) and glycosylated haemoglobin (HbA1c). The criteria vary depending on the country or organisation setting the standard. Whilst it is easy to find these references, there is dispute about the various cut off points, their sensitivity and specificity and the impact on patient care and outcomes.
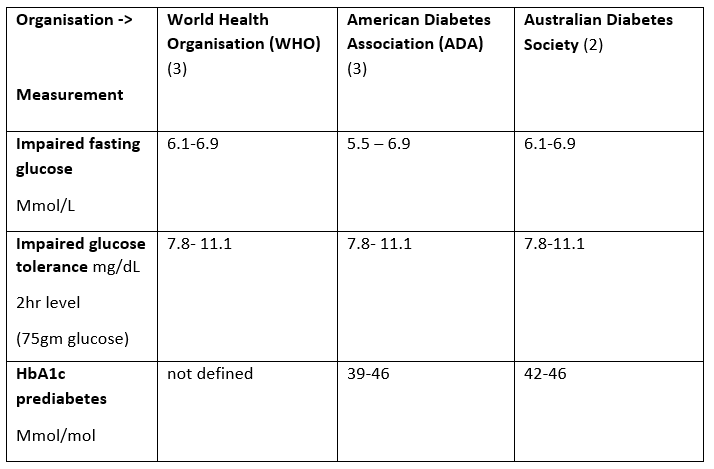
In Australia Type 2 diabetes is diagnosed with either a FBG (after 8 hours fast) ≥ 7 mmol/L, a 2-hour OGTT (with 75gm glucose load) ≥ 11.1 mmol/L or HbaA1c ≥ 48 mmol/mol. Asymptomatic patients require a second laboratory test as confirmation, whilst symptomatic patients do not (1). Symptoms include lethargy, polydipsia, polyuria, blurred vision, impaired sensation, frequent infections, and poor wound healing (1). A diagnosis of prediabetes is determined by any of a HbA1c of 42-46 Mmol/mol, impaired fasting glucose (IFG) (6.1-6.9 mmol/l) or impaired glucose tolerance (IGT) with a 2hr blood glucose of 7.8-11.1 mmol/L with OGTT (2).
Table 1 compares the definitions for prediabetes for the World Health Organisation definition, with the American and Australian Diabetes Society (3).
Table 1
Setting the optimal thresholds for both diabetes and prediabetes diagnosis is important because 30-40% of diabetics are undiagnosed, and microvascular and macrovascular complications are present in 25% of prediabetic patients (4).
In Bulgaria, a cross-sectional survey was conducted on 2231 subjects (both men and women who had at least one risk factor for diabetes) with a mean age 50.3 years to evaluate HbA1c as a diagnostic tool for prediabetes, IFG, IGT and diabetes. They found the optimal HbA1c cut off for diagnosing diabetes was 6.1% (43 mmol/mol) with a sensitivity of 86% and a specificity of 92%. Meanwhile they recommended a cut off point for pre-diabetes of 5.5% (37mmol/mol) with a sensitivity of 71% and a specificity of 64%. Comparatively using the ADA criteria for prediabetes of 5.7% (39mmol/mol) demonstrated a reduced sensitivity of 66% (with a specificity of 65%), whilst the ADA diabetes threshold with HbA1c 6.5% (48mmol/mol) had a lower sensitivity of 76% (with higher specificity of 94%) (4).
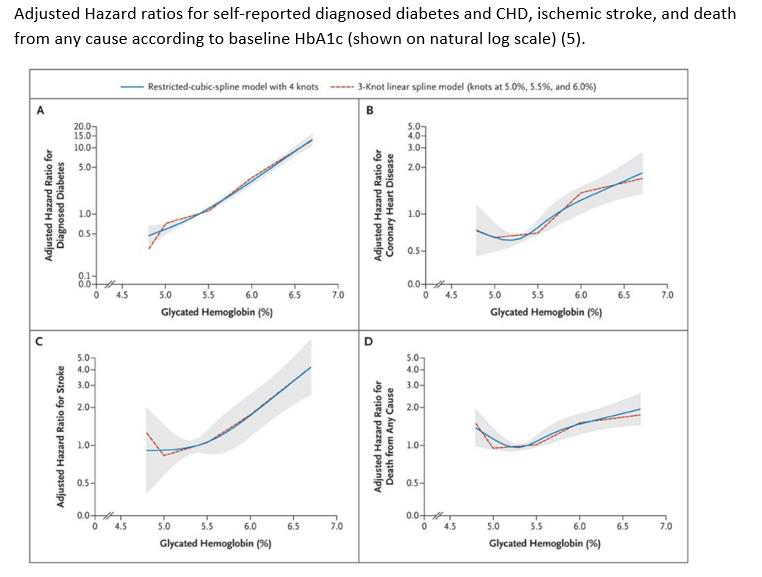
An important study is the ARIC (Atherosclerosis Risk in Communities study), which was a community prospective cohort study of 15792 middle aged adults (USA) and is one of the largest community studies of HbA1c and its correlation to the development of diabetes and cardiovascular disease. It found coronary heart disease risk increased from a HbA1c of 5.5 (37mmol/mol) with a HR 1.36 (CI 1.22-1.56) and this risk increased progressively with rising HbA1c levels (5).
A “rule-in, rule-out” approach to HbA1c has been suggested as the most appropriate with “rule” out HbA1c 5.5% and “rule-in” with Hba1c 7% (6).
Given the continuum of prediabetes and diabetes, and the fact that hyper-insulinemia increases complications in the absence of hyperglycemia, I believe lower cut offs for pre-diabetes and diabetes diagnosis are required. Ideally early diagnosis should be accompanied by ear dietary intervention, which ultimately would reduce costs on the healthcare system. Thus I flag a Hba1c of 5.5% and above with patients, and suggest intervention then.
Reference List
1. Royal Australian College of General Practitioners. Management of type 2 diabetes: A handbook for general practice [Internet}. 2020. Available from: https://www.racgp.org.au/getattachment/41fee8dc-7f97-4f87-9d90-b7af337af778/Management-of-type-2-diabetes-A-handbook-for-general-practice.aspx
2. Bell K, Shaw JE, Maple-Brown L, Ferris W, Gray S, Murfet G, et al. A position statement on screening and management of prediabetes in adults in primary care in Australia. Diabetes Research and Clinical Practice. 2020 Jun; 164:108188. DOI: https://doi.org/10.1016/j.diabres.2020.108188
3. Bansal N. Prediabetes diagnosis and treatment: A review. World Journal of Diabetes. 2015;6(2):296 doi: 10.4239/wjd.v6.i2.296
4. Tankova T, Chakaraova N, Dakovska L, Atanassova I. Assessment of HbA1c as a diagnostic tool in diabetes and prediabetes. Acta Diabetologica. 2011 Oct 2;49(5):371-8;24(4) doi.org/10.1007/s00592-011-0334-5
5. Selvin E, Steffes M, Zhu H, Matsushita K, Wagenknecht L, Pankow J et al. Glycated Hemoglobin, Diabetes, and Cardiovascular Risk in Nondiabetic Adults. N Engl J Med. 2010;362(9):800-811. DOI: 10.1056/NEJMoa0908359
6. Herman W, Cohen R. Racial and Ethnic Differences in the Relationship between HbA1c and Blood Glucose: Implications for the Diagnosis of Diabetes. The Journal of Clinical Endocrinology & Metabolism. 2012;97(4):1067-1072.